Weekly Biotech Watchlist: KDO (Tarcocimab), KZIA (Paxalisib)
Probability-weighted analysis of two clinical catalysts: tarcocimab (Phase 3, DR) and paxalisib (Phase 1b, TNBC), with estimated success rates and key risks.
Executive Summary
This watchlist highlights two upcoming late-stage and early-stage clinical catalysts across ophthalmology and oncology, spanning Phase 3 and Phase 1b development. Using a probability-weighted framework that integrates historical phase-transition base rates with mechanism validation, cross-indication learnings, and trial-level execution risk, we estimate the following probabilities of success:
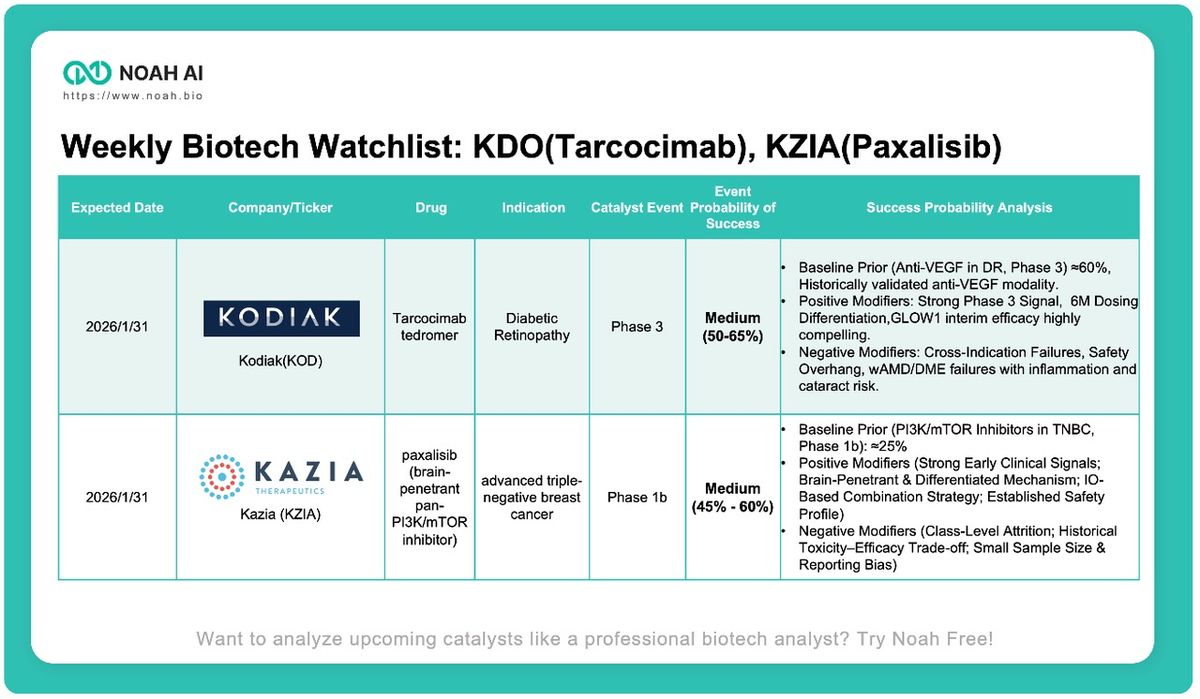
- KOD (Tarcocimab tedromer, Diabetic Retinopathy Phase 3): ~50–65%
A validated anti-VEGF mechanism and highly compelling interim efficacy support above-average late-stage odds, partially offset by platform-level safety overhang from prior retinal indications. - KZIA (Paxalisib, Advanced TNBC Phase 1b): ~45–60%
Meaningfully above historical PI3K/mTOR base rates due to unusually strong early efficacy signals and mechanistic differentiation, though still constrained by class-level attrition and limited sample size.
KOD (Kodiak Sciences) — Tarcocimab Tedromer
- Indication: Diabetic Retinopathy
- Stage: Phase 3
- Estimated Probability of Success: ~50–65%
- Relative Positioning: Above Average for Retinal Phase 3 Assets
Baseline Prior (Anti-VEGF in DR, Phase 3): ≈60%
- Anti-VEGF therapy is a highly validated modality in diabetic retinopathy and adjacent retinal diseases. Historically, approximately three out of five anti-VEGF agents entering Phase 3 for DR/DME have ultimately achieved FDA approval, implying an agent-level probability of success around ~60%.
- This baseline appropriately reflects program-level risk, incorporating not only biological validation but also late-stage execution and safety considerations.
Negative Modifiers — Cross-Indication Failures & Safety Overhang
- Despite the favorable modality precedent, tarcocimab carries material downside risk driven by its prior clinical history. The molecule failed in a Phase 2/3 wet AMD trial and demonstrated higher intraocular inflammation relative to aflibercept.
- More critically, the Phase 3 GLEAM/GLEAMER DME programs were discontinued due to lack of efficacy and an unexpected increase in cataract incidence.
- These late-stage failures in closely related retinal indications establish a non-trivial safety and durability risk, raising the possibility that similar issues could emerge in DR with longer exposure or broader patient enrollment.
Positive Modifiers — Compelling Phase 3 Efficacy & Dosing Differentiation
- Offsetting these concerns is exceptionally strong efficacy observed in the target indication. The GLOW1 interim analysis demonstrated a 41.1% response rate versus 1.4% for sham (p < 0.0001), representing a large and clinically convincing treatment effect.
- The validated VEGF-A mechanism materially reduces biological risk, while the tedromer-enabled 6-month dosing interval offers meaningful clinical differentiation by addressing treatment burden—a key adoption driver in DR.
Collectively, these factors support a probability of success above that of a typical late-stage retinal asset, albeit capped by unresolved platform-level safety risk.
KZIA (Kazia Therapeutics) — Paxalisib
- Indication: Advanced Triple-Negative Breast Cancer
- Stage: Phase 1b
- Estimated Probability of Success: ~45–60%
- Relative Positioning: Above PI3K/mTOR Class Averages
Baseline Prior (PI3K/mTOR Inhibitors in TNBC, Phase 1b): ≈25%
- PI3K/mTOR inhibitors in breast cancer have historically exhibited extremely high attrition. Among approximately 19 disclosed programs, only everolimus achieved approval—and exclusively in HR+ disease.
- With roughly 70% Phase II failure rates and the intrinsic resistance of TNBC to this pathway, a conservative baseline probability of success for a Phase 1b TNBC program is set at ~25%.
Negative Modifiers — Class-Level Attrition & Data Limitations
- The PI3K/mTOR class carries a >95% failure rate from Phase I to approval in breast cancer, with prior examples (e.g., buparlisib) underscoring the persistent toxicity–efficacy trade-off.
- In addition, current efficacy signals for paxalisib are derived from a very small cohort (n=6), introducing meaningful uncertainty related to selection bias, durability, and statistical robustness.
Positive Modifiers — Unusually Strong Early Signals & Mechanistic Differentiation
- Paxalisib demonstrates atypically strong early clinical activity for the class, including deep tumor regressions, an immune-complete response, and CTC reductions in most evaluable patients.
- Mechanistically, it is differentiated as the only reported brain-penetrant PI3K/mTOR inhibitor, expanding its therapeutic relevance in metastatic disease.
- The program is being evaluated in a modern pembrolizumab-based combination strategy, aligning with current TNBC treatment paradigms, while an established monotherapy safety database (>86 patients) reduces incremental safety uncertainty.
These factors collectively justify a probability of success meaningfully above historical class base rates, though still constrained by early-stage data maturity.
Disclosure: All analysis is conducted by Noah. This content is for informational purposes only and does not constitute investment or medical advice.